 Talk to Sales
Talk to Sales Benchmarks
View scores and output across OCR models spanning many document categories.
Want to run these evals on your own documents?
Talk to Sales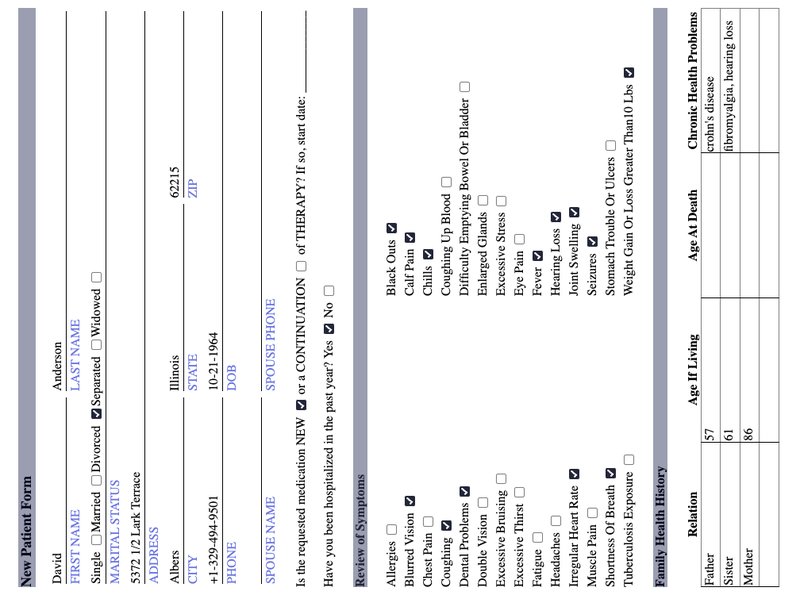
New Patient Form
David FIRST NAME Anderson LAST NAME
Single Married Divorced Separated Widowed
MARITAL STATUS
5372 1/2 Lark Terrace ADDRESS
Albers CITY Illinois STATE 62215 ZIP
+1-329-494-9501 PHONE 10-21-1964 DOB
SPOUSE NAME SPOUSE PHONE
Is the requested medication NEW or a CONTINUATION of THERAPY? If so, start date: _________.
Have you been hospitalized in the past year? Yes No
Review of Symptoms
Allergies
Blurred Vision
Chest Pain
Coughing
Dental Problems
Double Vision
Excessive Bruising
Excessive Thirst
Fatigue
Headaches
Irregular Heart Rate
Muscle Pain
Shortness Of Breath
Tuberculosis Exposure
Black Outs
Calf Pain
Chills
Coughing Up Blood
Difficulty Emptying Bowel Or Bladder
Enlarged Glands
Excessive Stress
Eye Pain
Fever
Hearing Loss
Joint Swelling
Seizures
Stomach Trouble Or Ulcers
Weight Gain Or Loss Greater Than 10 Lbs
Family Health History
| Relation | Age If Living | Age At Death | Chronic Health Problems |
|---|---|---|---|
| Father | 57 | crohn's disease | |
| Sister | 61 | fibromyalgia, hearing loss | |
| Mother | 86 |