 Talk to Sales
Talk to Sales Benchmarks
View scores and output across OCR models spanning many document categories.
Want to run these evals on your own documents?
Talk to Sales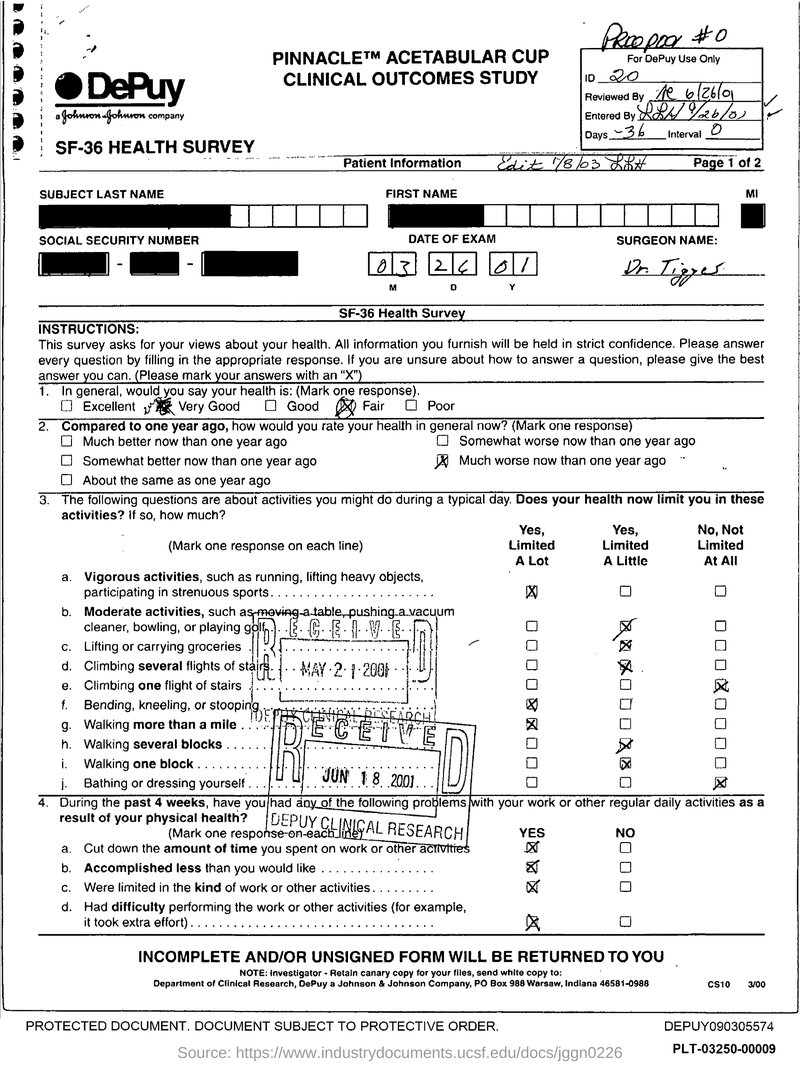

PINNACLE™ ACETABULAR CUP
CLINICAL OUTCOMES STUDY
SF-36 HEALTH SURVEY
Proopox #0
For DePuy Use Only
| ID | 20 | ||
| Reviewed By | R 6/26/01 | ||
| Entered By | R 9/26/01 | ||
| Days | -36 | Interval | 0 |
Patient Information
Edit 7/8/03 R&H
Page 1 of 2
SUBJECT LAST NAME
FIRST NAME
MI
SOCIAL SECURITY NUMBER
DATE OF EXAM
SURGEON NAME:
- - 03 26 01M D Y
Dr. Tigges
SF-36 Health Survey
INSTRUCTIONS:
This survey asks for your views about your health. All information you furnish will be held in strict confidence. Please answer every question by filling in the appropriate response. If you are unsure about how to answer a question, please give the best answer you can. (Please mark your answers with an "X")
1. In general, would you say your health is: (Mark one response).
Excellent
Very Good
Good
Fair
Poor
2. Compared to one year ago, how would you rate your health in general now? (Mark one response)
Much better now than one year ago
Somewhat worse now than one year ago
Somewhat better now than one year ago
Much worse now than one year ago
About the same as one year ago
3. The following questions are about activities you might do during a typical day. Does your health now limit you in these activities? If so, how much?
(Mark one response on each line)
Yes,Limited
A LotYes,
Limited
A LittleNo, Not
Limited
At All
a. Vigorous activities, such as running, lifting heavy objects, participating in strenuous sports.
b. Moderate activities, such as moving a table, pushing a vacuum cleaner, bowling, or playing golf.
c. Lifting or carrying groceries.
d. Climbing several flights of stairs.
e. Climbing one flight of stairs.
f. Bending, kneeling, or stooping.
g. Walking more than a mile.
h. Walking several blocks.
i. Walking one block.
j. Bathing or dressing yourself.
4. During the past 4 weeks, have you had any of the following problems with your work or other regular daily activities as a result of your physical health?
(Mark one response on each line)
a. Cut down the amount of time you spent on work or other activities YES NO
b. Accomplished less than you would like YES NO
c. Were limited in the kind of work or other activities. YES NO
d. Had difficulty performing the work or other activities (for example, it took extra effort). YES NO
INCOMPLETE AND/OR UNSIGNED FORM WILL BE RETURNED TO YOU
NOTE: Investigator - Retain canary copy for your files, send white copy to:
Department of Clinical Research, DePuy a Johnson & Johnson Company, PO Box 988 Warsaw, Indiana 46581-0988
CS10 3/00
PROTECTED DOCUMENT. DOCUMENT SUBJECT TO PROTECTIVE ORDER.
DEPUY090305574
Source: https://www.industrydocuments.ucsf.edu/docs/jggn0226
PLT-03250-00009