 Talk to Sales
Talk to Sales Benchmarks
View scores and output across OCR models spanning many document categories.
Want to run these evals on your own documents?
Talk to Sales Page 1 of 1
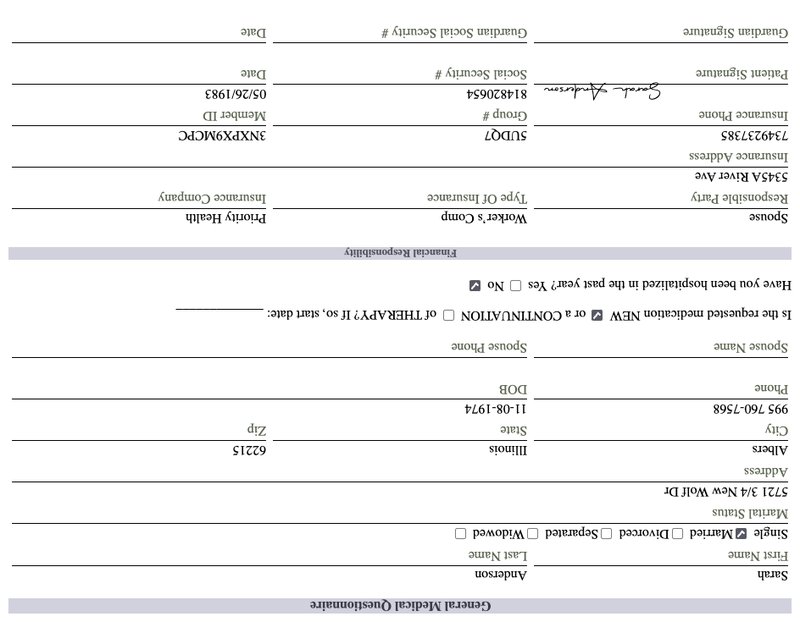
| Guardian Signature | Guardian Social Security # | Date |
| Patient Signature | Social Security # | Date |
| Sarah Anderson | 814820654 | 05/26/1983 |
| Insurance Phone | Group # | Member ID |
| 7349237385 | 5UDQ7 | 3NXPX9MCPC |
| Insurance Address | Type Of Insurance | Insurance Company |
| 5345A River Ave | Priority Health | |
| Responsible Party | Worker's Comp | Priority Health |
| Spouse |
Financial Responsibility
Have you been hospitalized in the past year? Yes No
Is the requested medication NEW or a CONTINUATION of THERAPY? If so, start date: ____________________
| Spouse Name | Spouse Phone |
| Phone | DOB |
| 995 760-7568 | 11-08-1974 |
| City | State |
| Albers | Illinois |
| Address | Zip |
| 5721 3/4 New Wolf Dr | 62215 |
| Marital Status | |
| Single Married Divorced Separated Widowed | |
| First Name | Last Name |
| Sarah | Anderson |
General Medical Questionnaire