 Talk to Sales
Talk to Sales Benchmarks
View scores and output across OCR models spanning many document categories.
Want to run these evals on your own documents?
Talk to Sales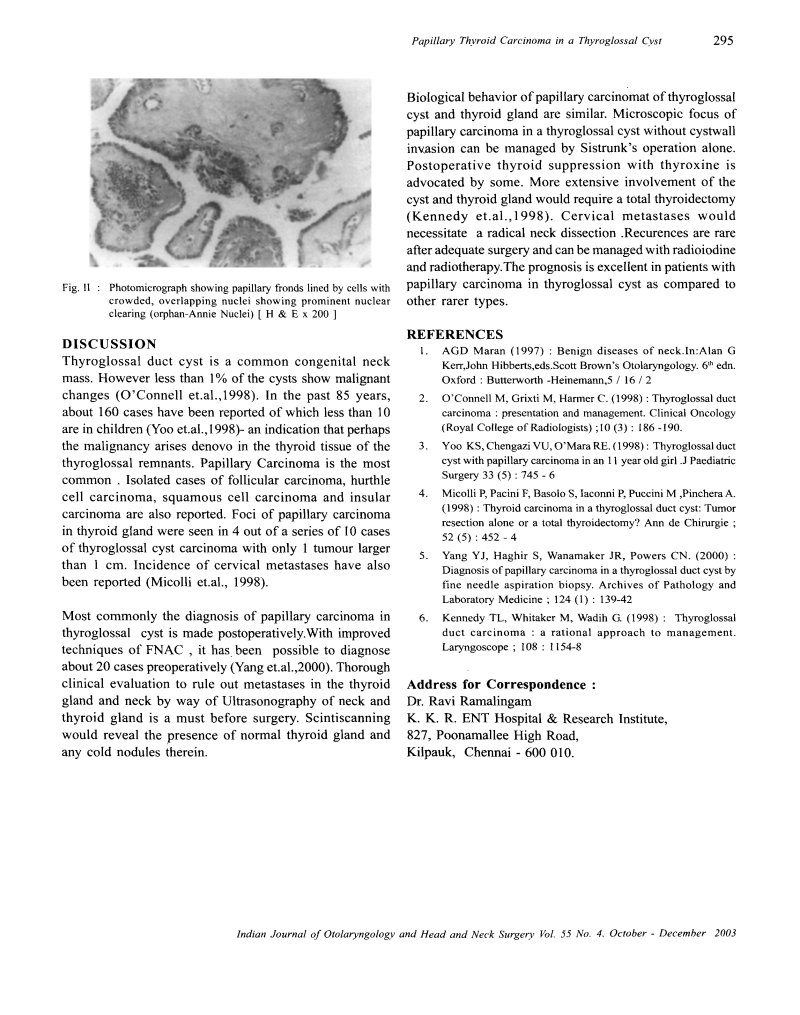
Papillary Thyroid Carcinoma in a Thyroglossal Cyst
295

Fig. II : Photomicrograph showing papillary fronds lined by cells with crowded, overlapping nuclei showing prominent nuclear clearing (orphan-Annie Nuclei) [ H & E x 200 ]
DISCUSSION
Thyroglossal duct cyst is a common congenital neck mass. However less than 1% of the cysts show malignant changes (O'Connell et al., 1998). In the past 85 years, about 160 cases have been reported of which less than 10 are in children (Yoo et al., 1998) - an indication that perhaps the malignancy arises denovo in the thyroid tissue of the thyroglossal remnants. Papillary Carcinoma is the most common. Isolated cases of follicular carcinoma, hurthle cell carcinoma, squamous cell carcinoma and insular carcinoma are also reported. Foci of papillary carcinoma in thyroid gland were seen in 4 out of a series of 10 cases of thyroglossal cyst carcinoma with only 1 tumour larger than 1 cm. Incidence of cervical metastases have also been reported (Micolli et al., 1998).
Most commonly the diagnosis of papillary carcinoma in thyroglossal cyst is made postoperatively. With improved techniques of FNAC, it has been possible to diagnose about 20 cases preoperatively (Yang et al., 2000). Thorough clinical evaluation to rule out metastases in the thyroid gland and neck by way of Ultrasonography of neck and thyroid gland is a must before surgery. Scintiscanning would reveal the presence of normal thyroid gland and any cold nodules therein.
Biological behavior of papillary carcinomat of thyroglossal cyst and thyroid gland are similar. Microscopic focus of papillary carcinoma in a thyroglossal cyst without cystwall invasion can be managed by Sistrunk's operation alone. Postoperative thyroid suppression with thyroxine is advocated by some. More extensive involvement of the cyst and thyroid gland would require a total thyroidectomy (Kennedy et al., 1998). Cervical metastases would necessitate a radical neck dissection. Recurences are rare after adequate surgery and can be managed with radioiodine and radiotherapy. The prognosis is excellent in patients with papillary carcinoma in thyroglossal cyst as compared to other rarer types.
REFERENCES
- AGD Maran (1997): Benign diseases of neck. In: Alan G Kerr, John Hibberts, eds. Scott Brown's Otolaryngology. 6 th edn. Oxford: Butterworth -Heinemann, 5 / 16 / 2
- O'Connell M, Grixti M, Harmer C. (1998): Thyroglossal duct carcinoma: presentation and management. Clinical Oncology (Royal College of Radiologists); 10 (3): 186 -190.
- Yoo KS, Chengazi VU, O'Mara RE. (1998): Thyroglossal duct cyst with papillary carcinoma in an 11 year old girl. J Paediatric Surgery 33 (5): 745 - 6
- Micolli P, Pacini F, Basolo S, Iaconni P, Puccini M, Pinchera A. (1998): Thyroid carcinoma in a thyroglossal duct cyst: Tumor resection alone or a total thyroidectomy? Ann de Chirurgie; 52 (5): 452 - 4
- Yang YJ, Haghir S, Wanamaker JR, Powers CN. (2000): Diagnosis of papillary carcinoma in a thyroglossal duct cyst by fine needle aspiration biopsy. Archives of Pathology and Laboratory Medicine; 124 (1): 139-42
- Kennedy TL, Whitaker M, Wadih G. (1998): Thyroglossal duct carcinoma: a rational approach to management. Laryngoscope; 108: 1154-8
Address for Correspondence :
Dr. Ravi Ramalingam
K. K. R. ENT Hospital & Research Institute,
827, Poonamallee High Road,
Kilpauk, Chennai - 600 010.
Indian Journal of Otolaryngology and Head and Neck Surgery Vol. 55 No. 4, October - December 2003